
Journal of Geographical Sciences >
Planning hierarchical hospital service areas for maternal care using a network optimization approach: A case study in Hubei, China
|
Tao Zhuolin (1990‒), PhD, specialized in spatial accessibility and optimization of public services, urban and regional development. E-mail: taozhuolin@bnu.edu.cn. |
Received date: 2021-11-29
Accepted date: 2022-06-09
Online published: 2022-12-25
Supported by
National Natural Science Foundation of China(41671497)
Improving maternal health is one of the Sustainable Development Goals. Hospital service areas (HSAs), which contain most hospitalization behaviors at the local scale, are crucial for health care planning. However, little attention has been given to HSAs for maternal care and the hierarchy structure. Considering Hubei, central China, as a case study, this study aims to fill these gaps by developing a method for delineating hierarchical HSAs for maternal care using a network optimization approach. The approach is driven by actual patient flow data and has an explicit objective to maximize the modularity. It also establishes the hierarchical structure of maternal care HSAs, which is fundamental for the planning of hierarchical maternal care and referral systems. In our case study, 45 secondary HSAs and 22 tertiary HSAs are delineated to achieve maximal modularity. The HSAs perform well in terms of indices such as the Localization Index and Market Share Index. Furthermore, there is a complementary relationship between secondary and tertiary hospitals, which suggests the need for referral system planning. This study can provide evidence for the validity of the HSA and the planning of maternal care HSAs in China. It also provides transferable methods for planning hierarchical HSAs in other developing countries.
TAO Zhuolin , CHENG Yang , BAI Lingyao , FENG Ling , WANG Shaoshuai . Planning hierarchical hospital service areas for maternal care using a network optimization approach: A case study in Hubei, China[J]. Journal of Geographical Sciences, 2022 , 32(12) : 2577 -2598 . DOI: 10.1007/s11442-022-2062-x
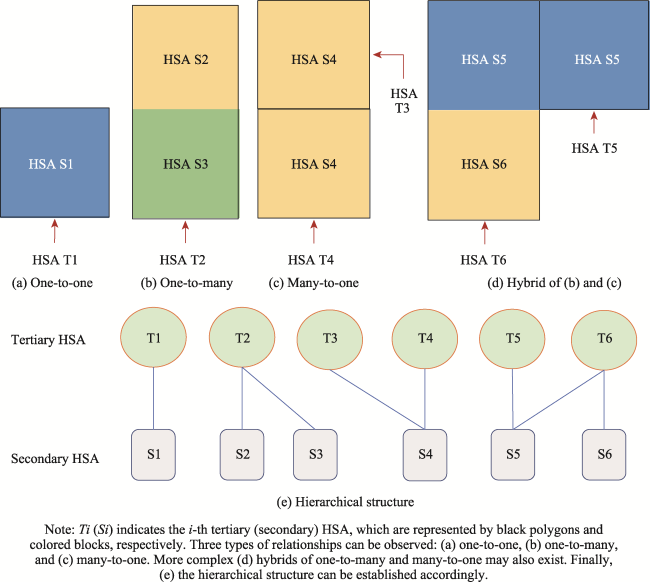
Figure 1 Illustration examples of various hierarchical structures of HSAs |
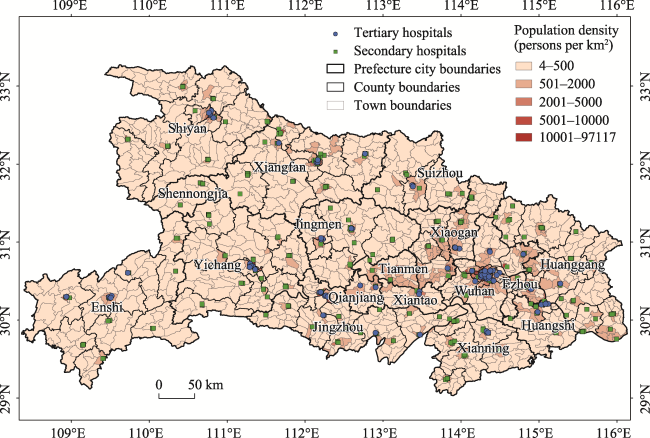
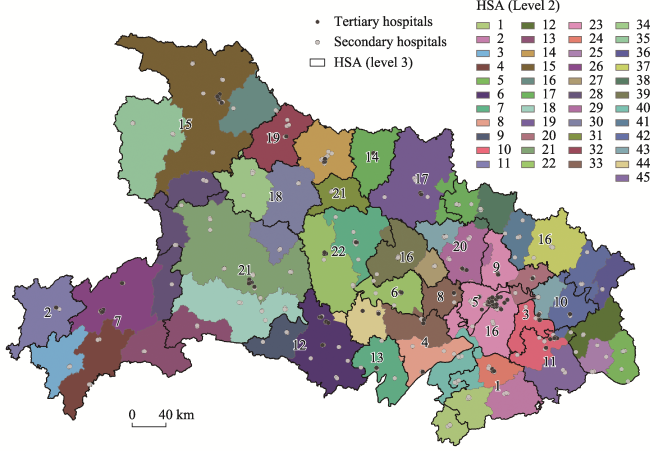
Figure 2 Distribution of population and tertiary and secondary hospitals in Hubei |
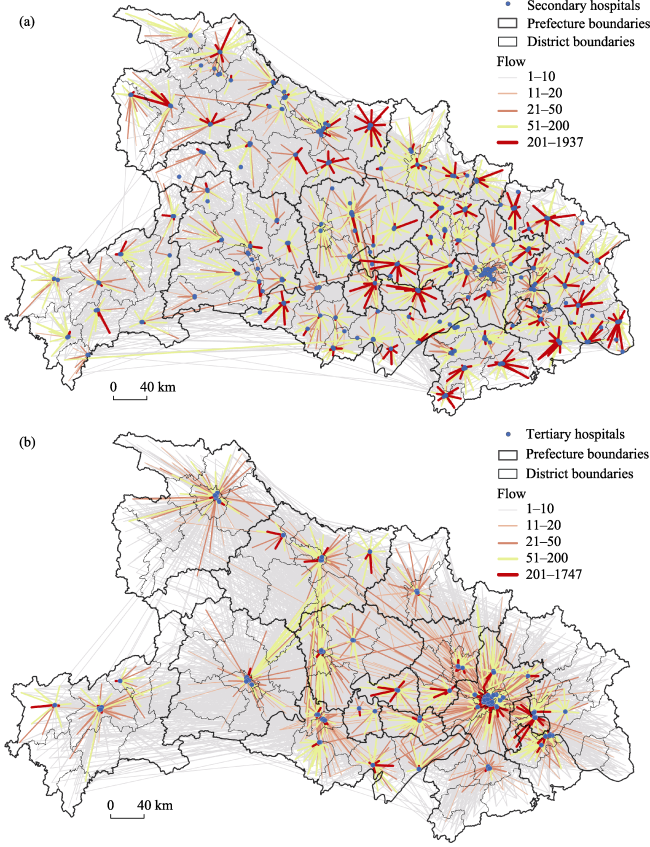
Figure 3 Distribution of maternal care patient flows to (a) secondary and (b) tertiary hospitals in Hubei |
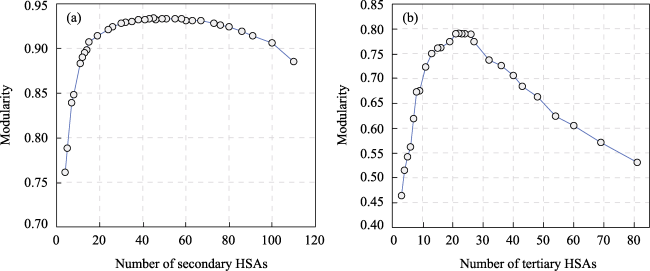
Figure 4 The relationships between the numbers of HSAs and modularity for secondary (left) and tertiary (right) hospitals |
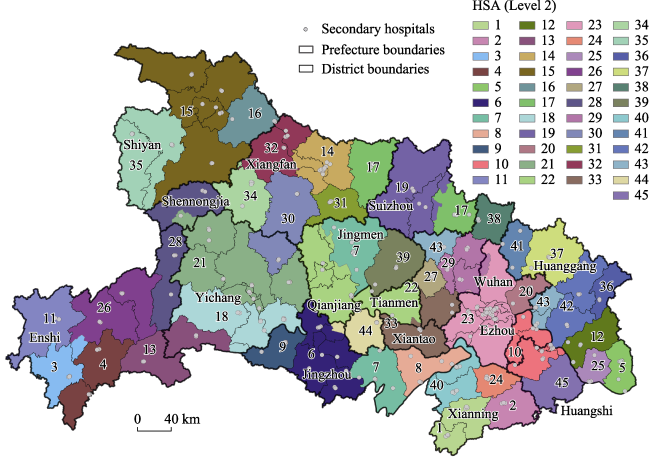
Figure 5 Secondary HSAs delineated by network optimization in Hubei |
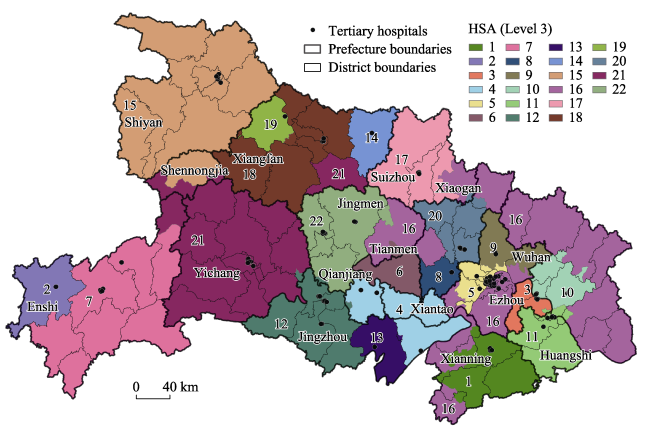
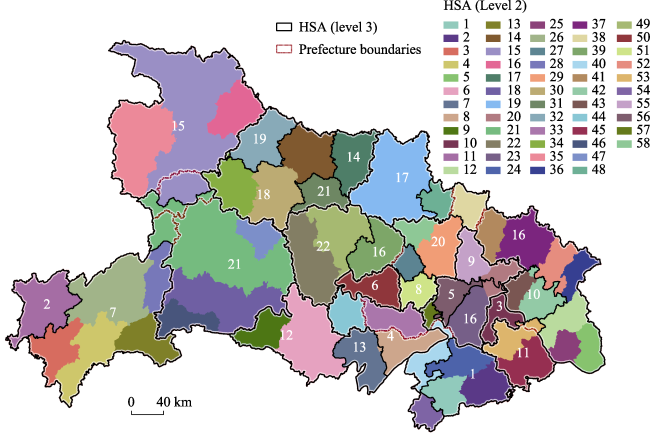
Figure 6 Tertiary HSAs delineated by network optimization in Hubei |
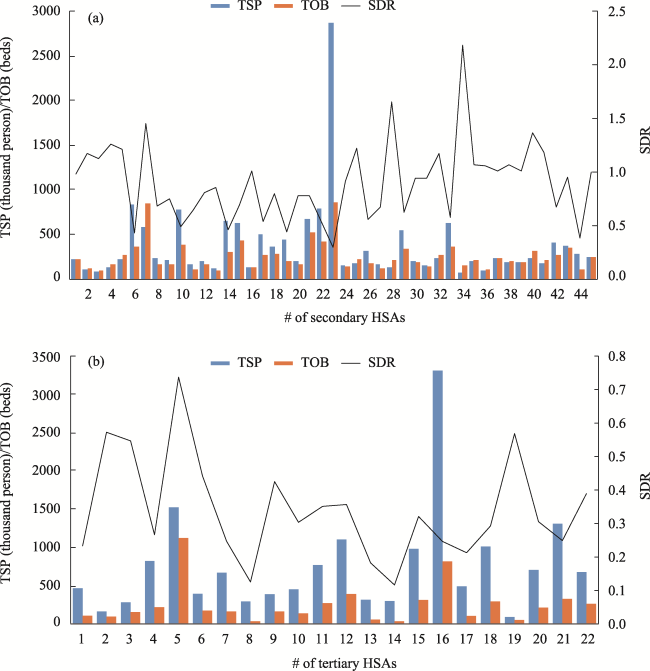
Figure 7 TSP, TOB and SDR of secondary and tertiary HSAs |
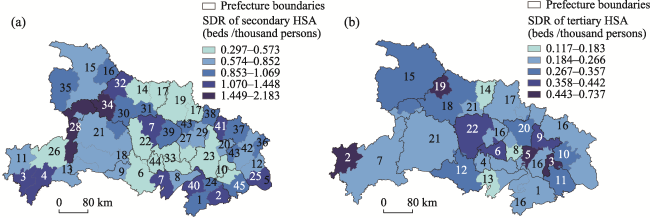
Figure 8 The distribution of SDR of secondary and tertiary HSAs in Hebei |
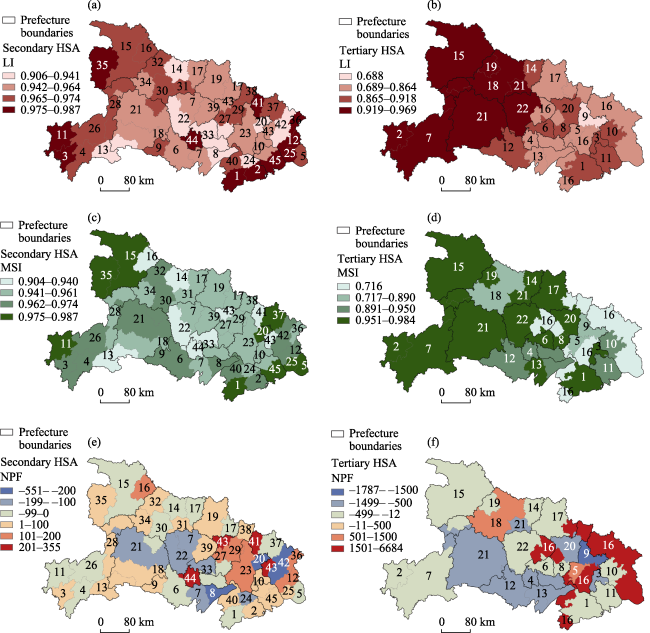
Figure 9 LI, MSI and NPI of secondary and tertiary HSAs in Hubei |
Figure 10 Tertiary HSAs overlaid with secondary HSAs in Hubei (Note: the labeled figures represent the numbers of tertiary HSAs) |
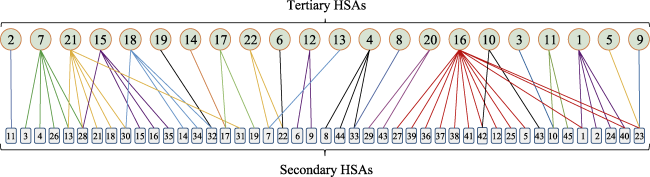
Figure 11 Mapping graph of the relationship between tertiary and secondary HSAs |
Figure 12 Adjusted tertiary and secondary HSAs based on consistency in Hubei |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
Healthy China Action Promotion Committee (HCAPC), 2019. Healthy China Action (2019-2030). Available at: http://www.gov.cn/xinwen/2019-07/15/content_5409694.htm. Accessed 3 June 2021. (in Chinese)
|
| [10] |
|
| [11] |
|
| [12] |
Hubei Provincial Bureau of Statistics (HPBS), 2018. Hubei Statistical Yearbook 2018. Beijing: China Statistics Press.
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
State Council of the People’s Republic of China (SC), 2015. Guiding opinions on propelling the building of a hierarchical diagnosis and treatment system. Beijing. Available at: http://www.gov.cn/zhengce/content/ 2015-09/11/content_10158.htm. Accessed 3 June 2021. (in Chinese)
|
| [35] |
UN, 2013. 2013 Fact sheet of Millennium Development Goals and beyond 2015. Available at: https://www. un.org/millenniumgoals/pdf/Goal_5_fs.pdf. Accessed 3 June 2021.
|
| [36] |
UN, 2015. The Millennium Development Goals Report 2015. Available at: https://www.undp.org/content/ undp/en/home/librarypage/mdg/the-millennium-development-goals-report-2015.html. Accessed 3 June 2021.
|
| [37] |
UN, 2020. Sustainable Development Goals. Available at: https://www.un.org/sustainabledevelopment/. Accessed 3 June 2021.
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
World Health Organisation (WHO), 1991. Sundsvall statement on supportive environments for health. 3rd International Conference on Health Promotion, 9-15 June 1991, Sundsvall, Sweden. Available at: https://www.who.int/healthpromotion/conferences/previous/sundsvall/en/.
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}