
Journal of Geographical Sciences >
Spatiotemporal patterns of the daily relative risk of COVID-19 in China
|
Cheng Changxiu, Professor, specialized in spatiotemporal data analysis. E-mail: chengcx@bnu.edu.cn |
Received date: 2021-03-25
Accepted date: 2021-05-14
Online published: 2021-09-25
Supported by
National Key Research and Development Plan of China(2019YFA0606901)
The Second Tibetan Plateau Scientific Expedition and Research Program (STEP)(2019QZKK0608)
The Strategic Priority Research Program of the Chinese Academy of Sciences(XDA23100303)
The Fundamental Research Funds for the Central Universities(2019NTST01)
Copyright
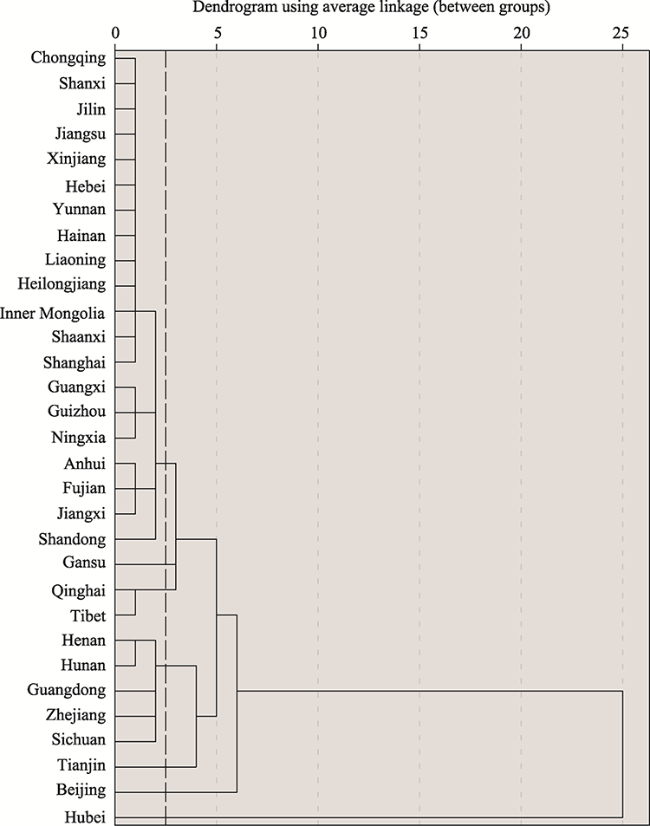
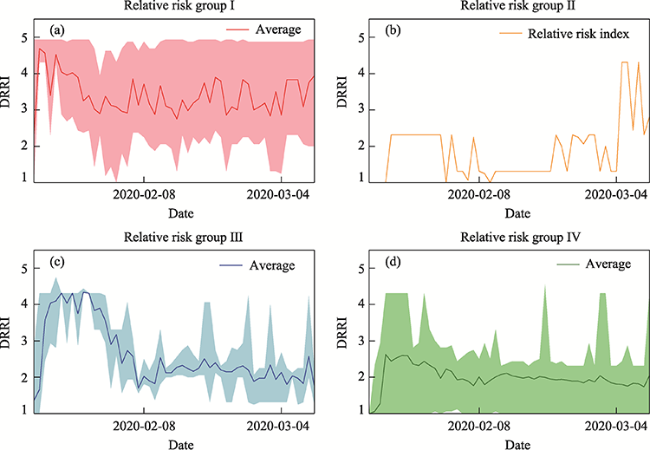
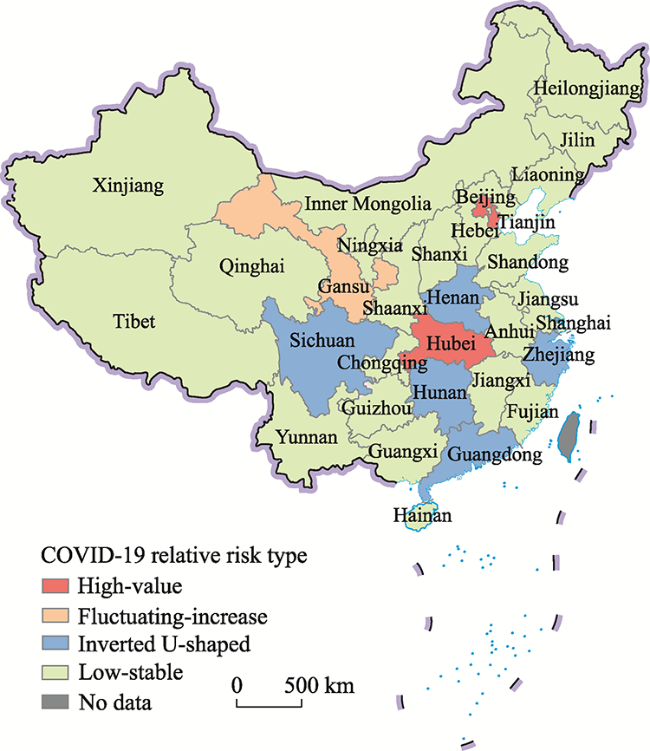
The coronavirus disease 2019 (COVID-19) pandemic continues to threaten lives and the economy around the world. Estimating the risk of COVID-19 can help in predicting spreading trends, identifying risk areas, and making public health decisions. In this study, we proposed a comparative risk assessment method to estimate comprehensive and dynamic COVID-19 risks by considering the pandemic severity and the healthcare system pressure and then employing the z-order curve and fractal theory. We took the COVID-19 cases from January 19-March 10, 2020 in China as our research object. The results and analysis revealed that (1) the proposed method demonstrated its feasibility to assess and illustrate pandemic risk; (2) the temporal patterns of the daily relative risk indices of 31 provinces were clustered into four groups (high-value, fluctuating-increase, inverted U-shaped, and low-stable); (3) the spatial distribution of the relative pandemic risk indicated a significant circular pattern centered on Hubei Province; and (4) healthcare system capacity is the key to reducing relative pandemic risk, and cases imported from abroad should be given more attention. The methods and results of this study will provide a methodological basis and practical guidance for regional pandemic risk assessment and public health decision-making.
Key words: COVID-19; risk assessment; spatiotemporal patterns; z-order curve; fractal
CHENG Changxiu , JIANG Yifan , SONG Changqing , SHEN Shi , WU Yunfeng , ZHANG Tianyuan . Spatiotemporal patterns of the daily relative risk of COVID-19 in China[J]. Journal of Geographical Sciences, 2021 , 31(7) : 1039 -1058 . DOI: 10.1007/s11442-021-1884-2
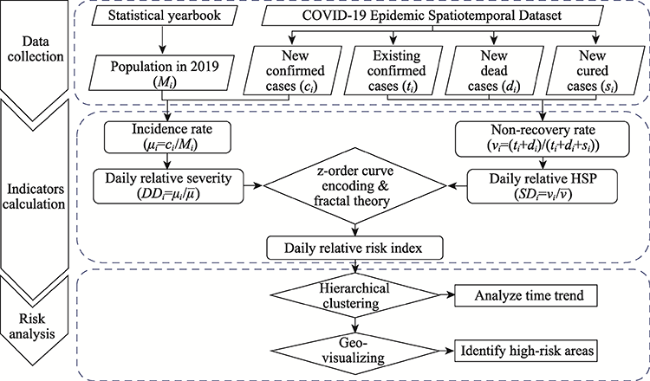
Figure 1 Flow chart of daily relative risk index construction and analysis |
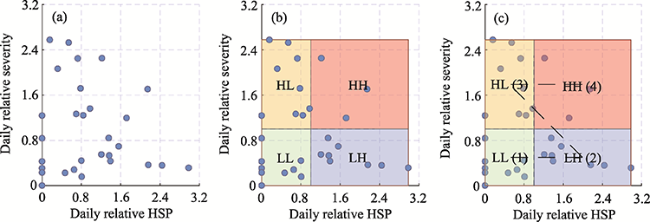
Figure 2 Risk coordinates and z-order curve encoding (Note: HH represents high relative severity and high relative HSP; HL represents high relative severity and low relative HSP; LH represents low relative severity and high relative HSP; LL represents low relative severity and low relative HSP.) |
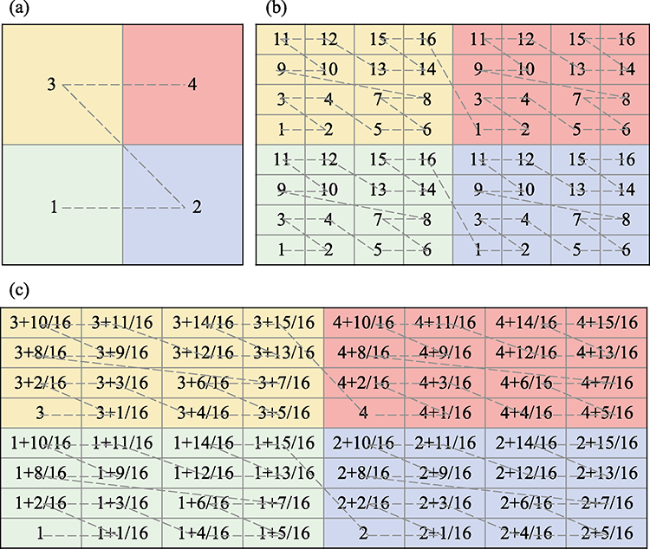
Figure 3 Subdivisions of risk coordinates and calculation of DRRIs |
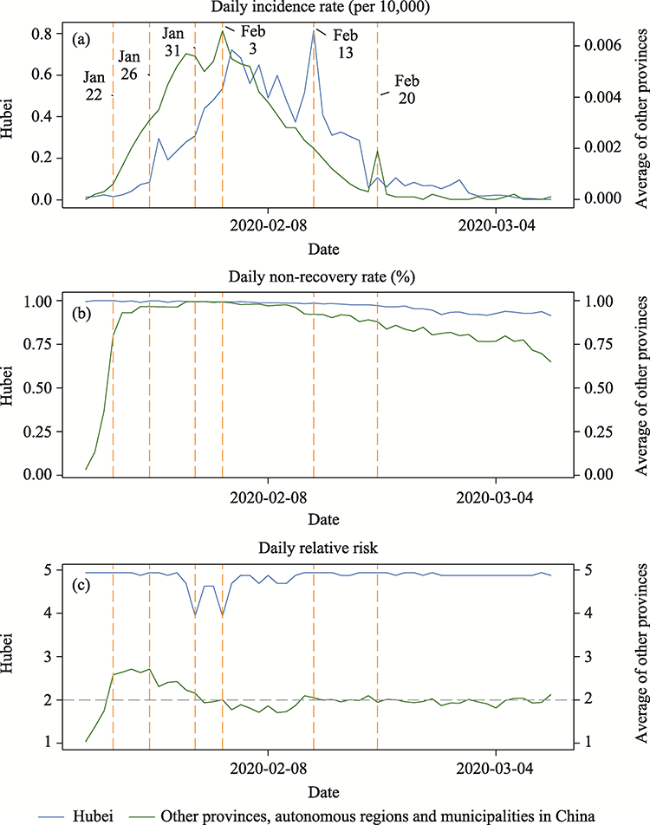
Figure 4 Temporal trends of the pandemic and DRRI in Hubei Province and other provinces, autonomous regions and municipalities in China |
Figure 5 Hierarchical clusters of the DRRIs of 31 provinces, autonomous regions and municipalities in China |
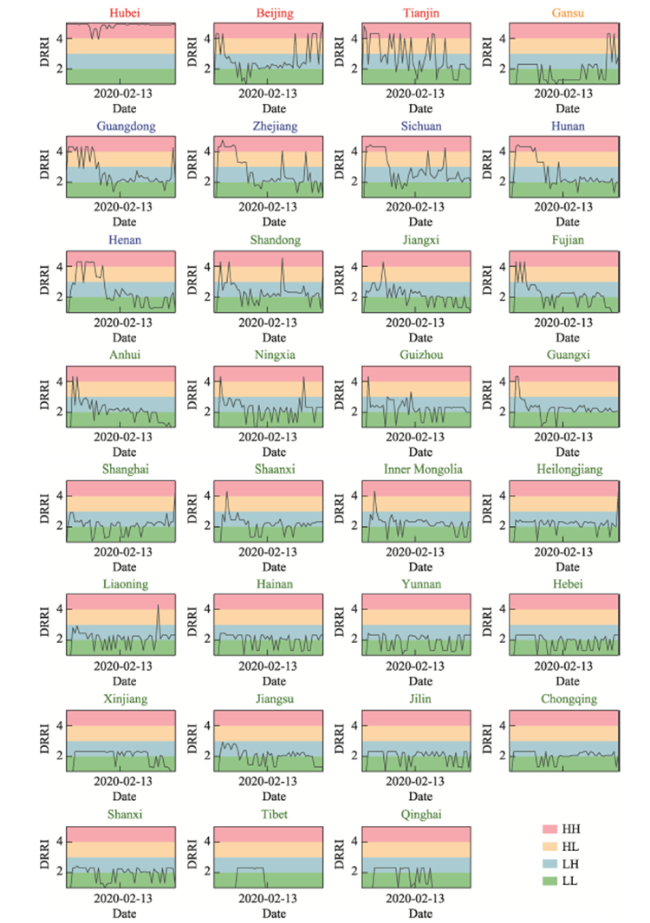
Figure 6 DRRI of 31 provinces, autonomous regions and municipalities in China (HH: High daily relative severity and high daily relative HSP; HL: High daily relative severity and low daily relative HSP; LH: Low daily relative severity and high daily relative HSP; LL: Low daily relative severity and low daily relative HSP) |
Figure 7 Temporal patterns of the four aggregated risk groups |
Figure 8 Spatial patterns of the four risk groups in China |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
CGTN, 2020. Last two temporary hospitals in Wuhan close, finalizing phaseout. https://news.cgtn.com/news/2020-03-10/Last-two-temporary-hospitals-in-Wuhan-close-finalizing-phaseout-OKuAJwwXsI/index.html. Accessed 7 Sept 2020.
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
Chinese Center for Disease Control and Prevention (CCDC), 2020. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)-China, 2020. http://weekly.chinacdc.cn/en/article/id/e53946e2-c6c4-41e9-9a9b-fea8db1a8f51. Accessed 7 Sept 2020.
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
INFORM Epidemic Risk Index. https://drmkc.jrc.ec.europa.eu/inform-index/INFORM-Risk/INFORM-Epidemic-Risk-Index.
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
World Health Organization (WHO), 2021. COVID-19 Weekly Epidemiological Update. https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19-18-may-2021. Accessed 24 May 2021.
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
|
| [54] |
|
| [55] |
|
| [56] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}