
Journal of Geographical Sciences >
Comparison of spatio-temporal transmission characteristics of COVID-19 and its mitigation strategies in China and the US
|
Feng Zhiming (1963‒), PhD and Professor, specialized in geography of natural resources and sustainable utilization of land resources. E-mail: fengzm@igsnrr.ac.cn |
Received date: 2020-09-10
Accepted date: 2020-10-13
Online published: 2021-02-25
Supported by
Strategic Priority Research Program of Chinese Academy of Sciences(XDA20010203)
Second Tibetan Plateau Scientific Expedition and Research Program (STEP)(2019QZKK1006)
Copyright
Investigating the spatio-temporal transmission features and process of novel coronavirus disease 2019 (COVID-19) mitigation strategies are of great practical significance to understand the development of COVID-19 and establish international cooperation for prevention and control. In this paper, the cumulative number of confirmed cases, number of confirmed cases per day and cumulative number of deaths, were used to compare transmission paths, outbreaks timelines, and coping strategies of COVID-19 in China and the US. The results revealed that: first, the COVID-19 outbreaks in both China and the US exhibited a 6-week initiation stage. In China, the COVID-19 erupted in late January. It lasted only a short period of time and was almost completely contained within 6-8 weeks. But the COVID-19 erupted in early March in the US and was still in the peak or post-peak stage. Second, in China, the COVID-19 emerged in Wuhan and spread to other regions of Hubei Province and then nationwide, exhibiting a cross(“+”)-shaped of spread with Wuhan city as the center. Importantly, the COVID-19 in China had a large concentration and there were no national outbreaks. In contrast, the COVID-19 in the US first spread through New York and the western and eastern coasts but has since emerged throughout the entire country. Third, the lack of emergency response planning in both countries in the early stage (about 6-week) hampered COVID-19 prevention. However, actively high-pressure prevention and control measures were used to basically control COVID-19 in early March in China. And then China has gradually resumed business and production activities. Unfortunately, the US government missed the best opportunity to contain the epidemic. Faced with the choice between economic recovery and coronavirus containment, the US removed the quarantine and restriction measures too early. The COVID-19 is continuing to spread in the country and blossom everywhere, still showing no signs of receding.
Key words: COVID-19; spatio-temporal transmission; timelines; mitigation strategy; China; the US
FENG Zhiming , XIAO Chiwei , LI Peng , YOU Zhen , YIN Xu , ZHENG Fangyu . Comparison of spatio-temporal transmission characteristics of COVID-19 and its mitigation strategies in China and the US[J]. Journal of Geographical Sciences, 2020 , 30(12) : 1963 -1984 . DOI: 10.1007/s11442-020-1822-8
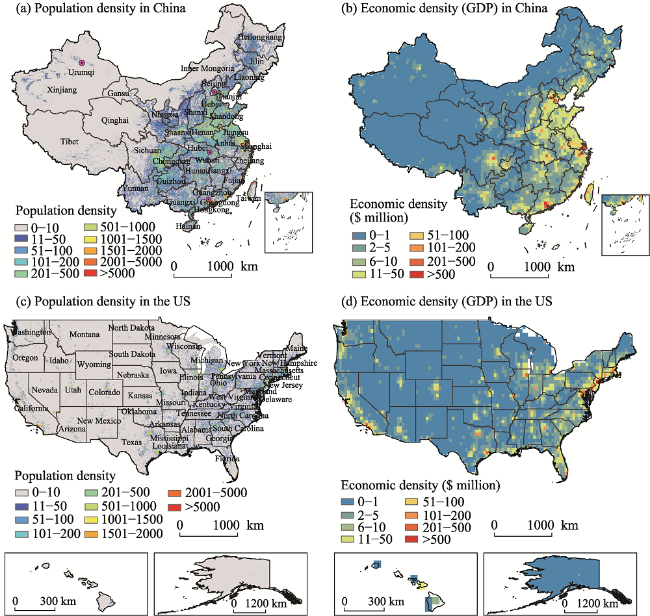
Figure 1 Distributions of population (2018) and economic densities (2020) in China and the US |
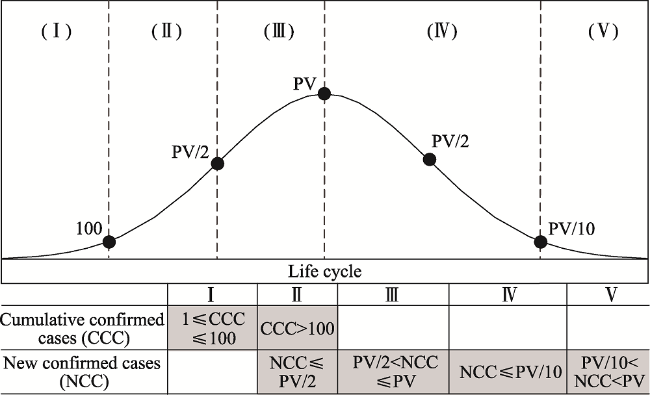
Figure 2 The five stages of COVID-19 outbreak |
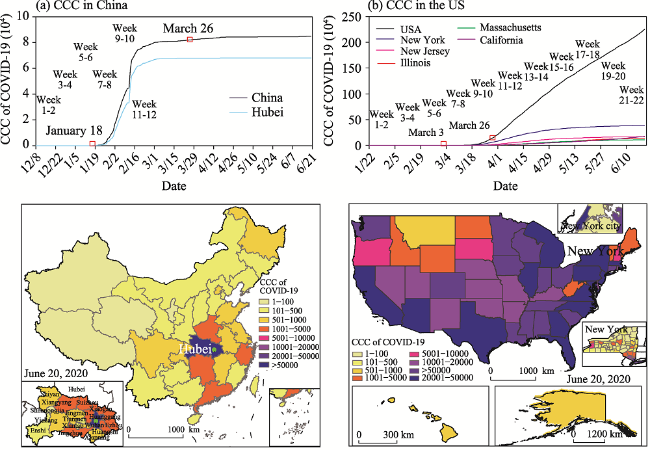
Figure 3 Comparisons of the CCC of COVID-19 between China and the US |
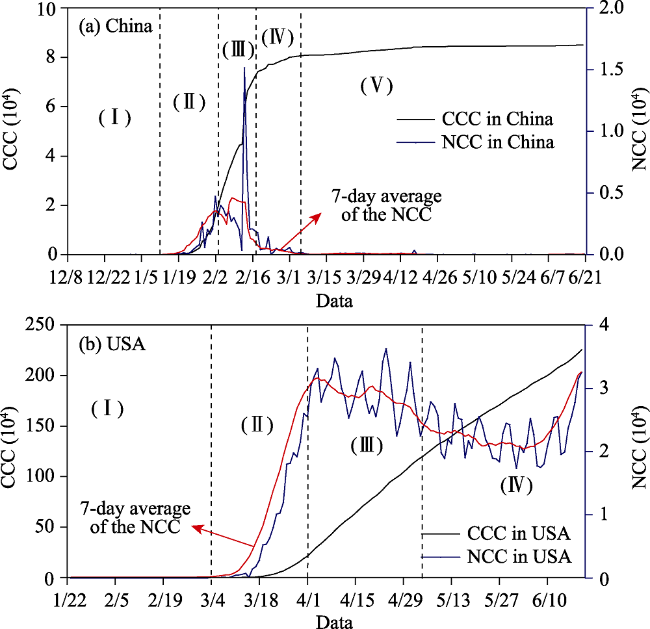
Figure 4 Comparisons of the NCC and CCC of COVID-19 over time between (a) China and (b) the US |
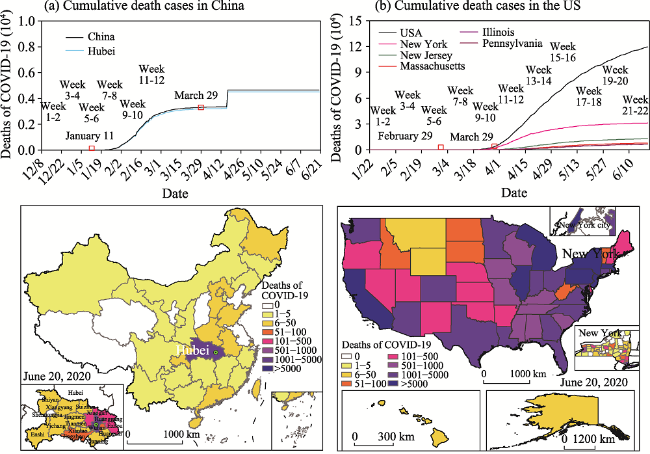
Figure 5 Comparisons of the cumulative deaths of COVID-19 between China and the US |
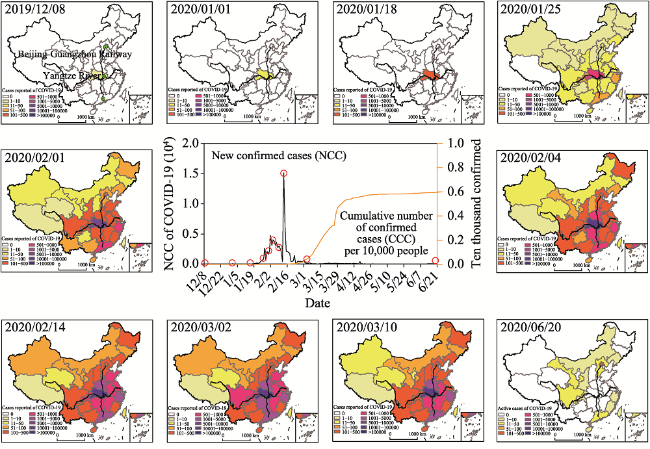
Figure 6 Spatio-temporal dynamics process of the CCC as well as NCC and CCC per 10,000 people of COVID-19 at critical time points in China and its provinces |
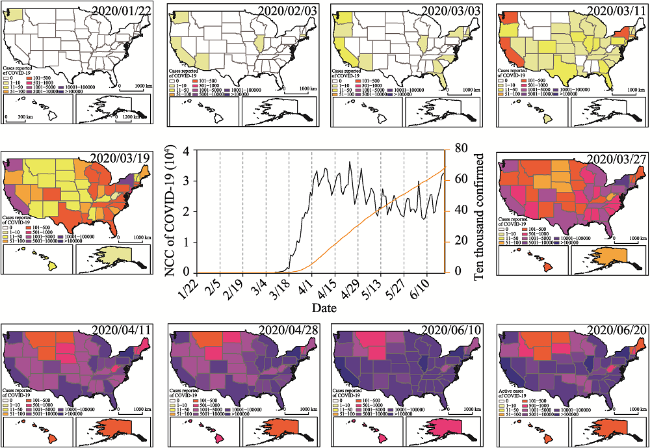
Figure 7 Spatio-temporal dynamics process of the CCC as well as NCC and CCC per 10,000 people of COVID-19 at critical time points in the US and its states |
Table 1 Dynamics of the COVID-19 CCC at critical time points in China and the US |
| China | the US | ||||||
|---|---|---|---|---|---|---|---|
| Timeline | Interval days | CCC | Timeline | Interval days | CCC | ||
| 1 | 2019/12/8 | - | 1 | 1 | 2020/1/22 | - | 1 |
| 10 | 2020/1/1 | 25 | 27 | 10 | 2020/2/3 | 13 | 11 |
| 100 | 2020/1/18 | 17 | 121 | 100 | 2020/3/3 | 29 | 18 |
| 1000 | 2020/1/25 | 7 | 1409 | 1000 | 2020/3/11 | 8 | 1285 |
| 10,000 | 2020/2/1 | 7 | 11,901 | 10,000 | 2020/3/19 | 8 | 13,748 |
| 20,000 | 2020/2/4 | 4 | 23,718 | 100,000 | 2020/3/27 | 8 | 101,962 |
| 40,000 | 2020/2/10 | 6 | 42,372 | 500,000 | 2020/4/11 | 15 | 526,776 |
| 60,000 | 2020/2/14 | 4 | 66,376 | 1,000,000 | 2020/4/28 | 17 | 1,012,582 |
| 80,000 | 2020/3/2 | 17 | 80,177 | 2,000,000 | 2020/6/10 | 43 | 2,000,464 |
| Active cases | 2020/6/20 | - | 403 | Active cases | 2020/6/20 | - | 1,235,657 |
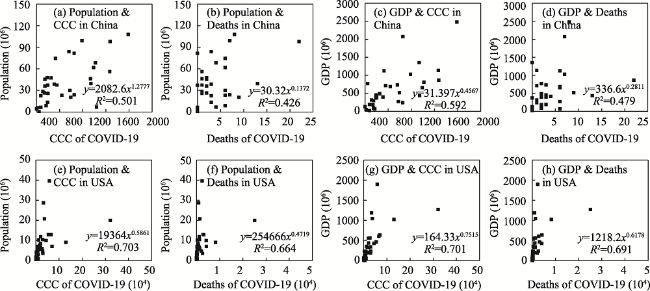
Figure 8 Correlations between the CCC and population, cumulative deaths and population, the CCC and GDP, cumulative deaths and GDP in China (excluding Hubei Province) and the US |
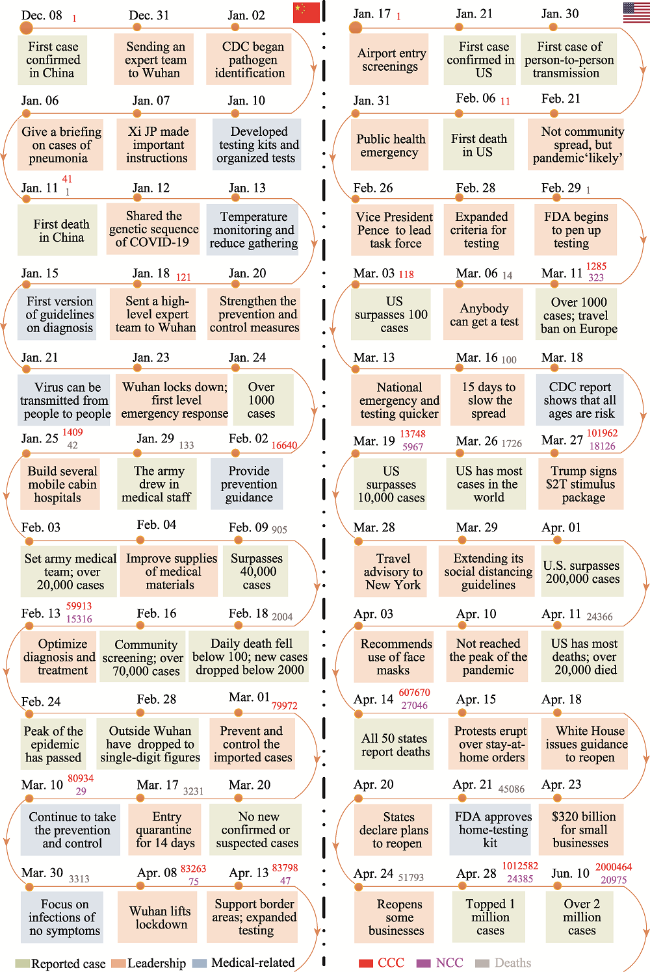
Figure 9 Timelines of COVID-19 developments in China and the US |
COVID-19 data products are freely available from the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. We also thank the editors and two anonymous reviewers for their valuable comments that helped to improve this manuscript.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
National Health Commission of the People’s Republic of China (NHCPRC), 2020. COVID-19 epidemic situation up to 24:00 on March 8th http://www.nhc.gov.cn/xcs/yqtb/202003/f2c83db9f73d4be5be0dc96af731813c.shtml/.
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
United Nations, 2016. Sustainable Development Goals: 17 Goals to Sustain Our World. New York: United Nations. http://www.un.org/sustainabledevelopment/sustainable-development-goals/.
|
| [32] |
|
| [33] |
|
| [34] |
World Health Organization (WHO), 2020. Coronavirus Disease (COVID-2019) Situation Reports. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/.
|
| [35] |
|
| [36] |
Xinhua News Agency (XNA), 2020. COVID-19 is urged by the UN Secretary General to do everything possible to contain the outbreak. http://www.xinhuanet.com/2020-02/29/c_1125642849.htm/.
|
| [37] |
|
| [38] |
|
| [39] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}