
Journal of Geographical Sciences >
Regional differences in the health status of Chinese residents: 2003-2013
Author: Zhao Xueyan (1971-), Professor, specialized in ecological economics. E-mail: zhaoxy@nwnu.edu.cn
Received date: 2017-06-12
Accepted date: 2017-08-02
Online published: 2018-06-20
Supported by
National Natural Science Foundation of China, No.41661115, No.41361106
The Open Fund of Key Laboratory of Ecohydrology of Inland River Basin, Chinese Academy of Sciences, No.KLEIRB-2S-16-03
Copyright
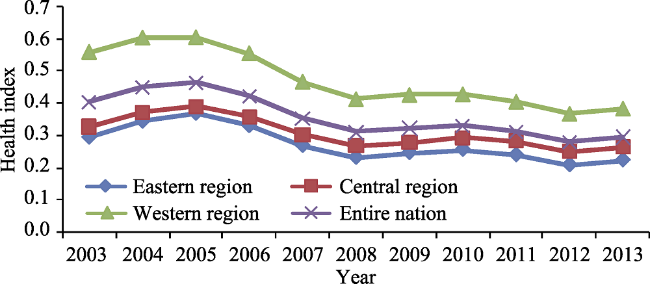
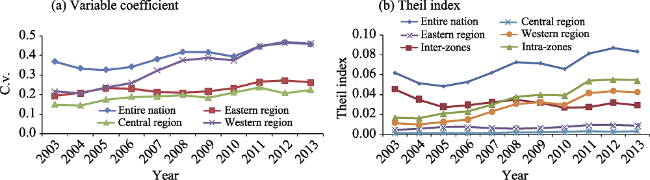
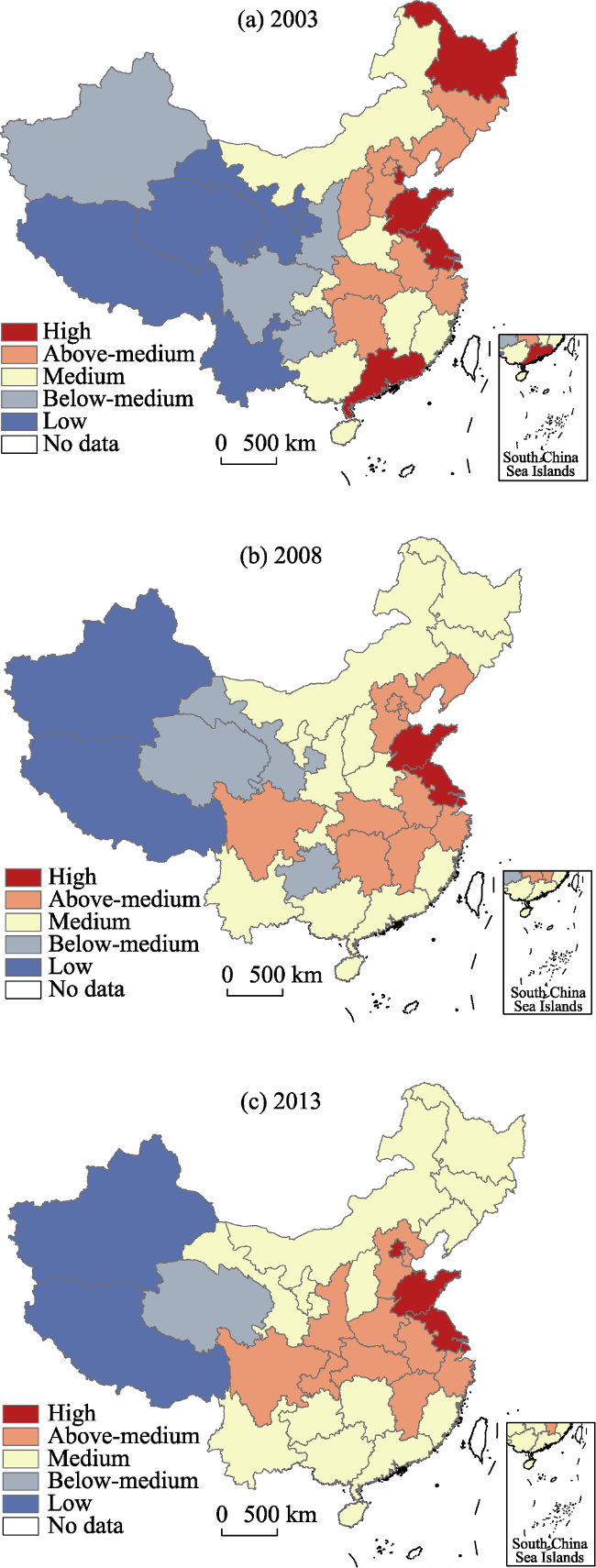
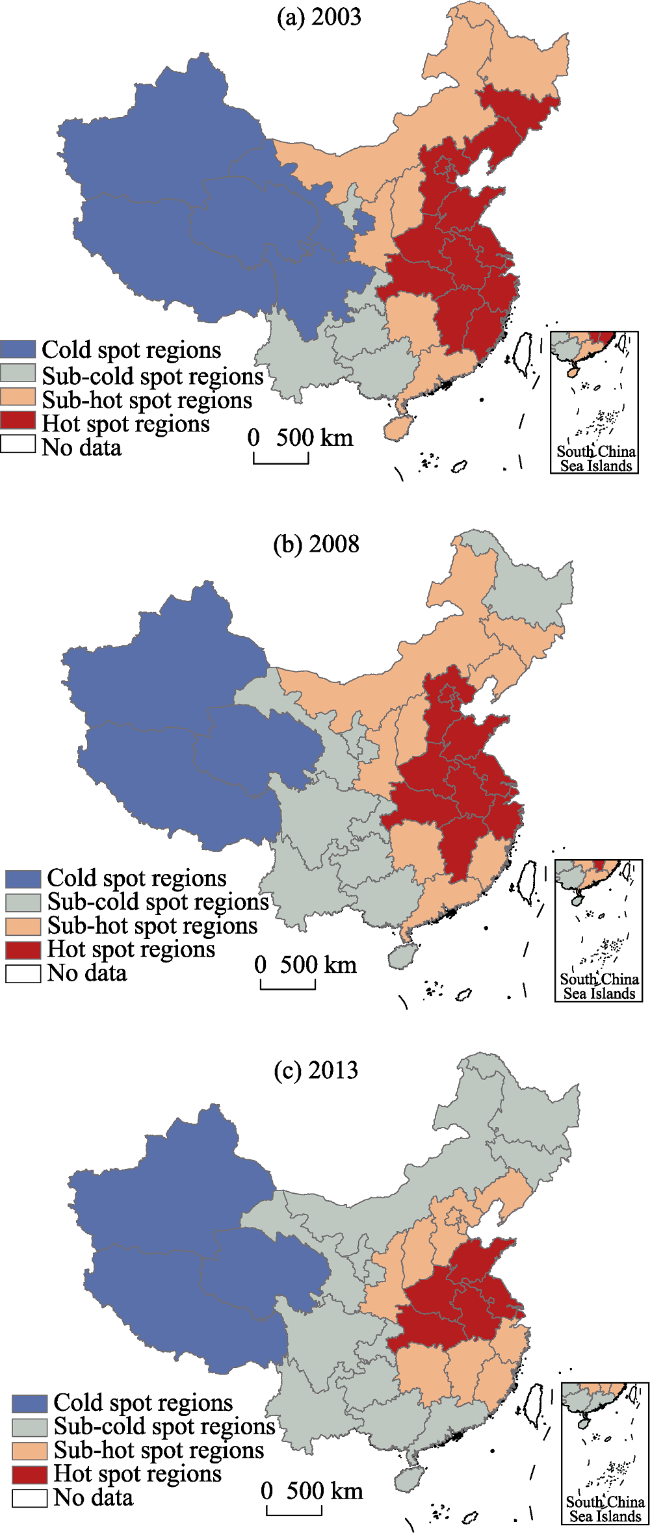
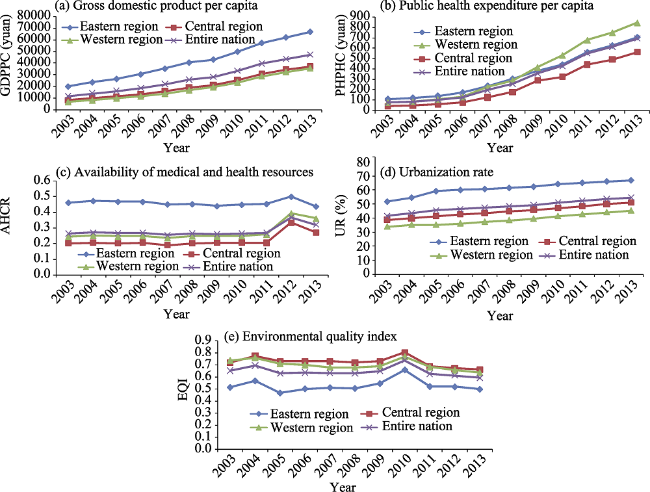
Health inequality is an increasing concern worldwide. Using the coefficient of variation, Theil index, exploratory spatial data analysis, and spatial panel econometric model, we examined the regional inequality, spatio-temporal dynamic patterns, and key factors in the health status of Chinese residents from 2003 to 2013. We found that China’s residential health index (RHI) decreased from 0.404 to 0.295 in 2003-2013 at an annual rate of 2.698%. Spatially, resident health status, based on the RHI, has improved faster in the western region than in the eastern and central regions. Inequality in resident health status continued to increase between 2003 and 2013; inequality between regions decreased, but health status inequality expanded within regions. Furthermore, disparities in health status grew faster in western regions than in the eastern and central regions. The spatial distribution of resident health status formed a “T-shaped” pattern across China, decreasing from east to center then to the west with a symmetric decrease north and south. Using the change in Moran’s I from 2003 to 2008 and 2013, we found that the distribution of resident health status across China has narrowed. All the hot spots and cold spots have decreased, but they are also stable. Resident health status formed a stable cold spot in the western regions, while the east coastal area formed a stable hot spot. Selected explanatory variables have significant direct impacts on resident health status in China: increasing per capita GDP, per capita spending on health, and urbanization, and improving environmental quality all lead to better resident health status. Finally, we highlight the need for additional research on regional inequality of resident health status across multiple time, spatial, and factor domains.
Key words: residents; health status; regional inequity; influencing factors; China
ZHAO Xueyan , WANG Weijun , WAN Wenyu . Regional differences in the health status of Chinese residents: 2003-2013[J]. Journal of Geographical Sciences, 2018 , 28(6) : 741 -758 . DOI: 10.1007/s11442-018-1502-0
Figure 1 Trends in the residents’ health index (RHI) in China from 2003 to 2013 |
Figure 2 Regional differences in resident health status in China from 2003-2013 based on (a) the variable coefficient and (b) the Theil index |
Figure 3 The spatial distribution of resident health status in China for 2003 (a), 2008 (b), and 2013 (c) |
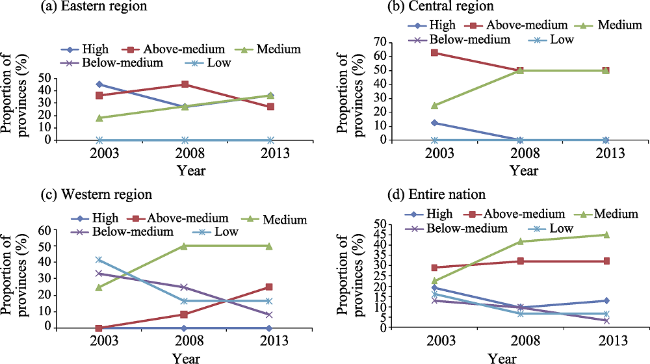
Figure 4 Resident health status in different parts of China, eastern region (a), central region (b), western region (c), and the entire nation (d), from 2003 to 2013 |
Figure 5 The spatio-temporal dynamics of the resident health status in China based on local spatial relationships in 2003 (a), 2008 (b), and 2013 (c) |
Figure 6 Trends in key human factors from 2003 to 2013, GDPPC is gross domestic product per capita (a), PCPHE is per capita public health expenditure (b), AHCR is accessibility of health care resources (c), UR is urbanization rate (d), and EQI is environmental quality index (e) |
Table 1 Pearson correlation coefficients between RHIs and key human factors |
| Variable | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| GDPPC | -0.508** | -0.486** | -0.422** | -0.453** | -0.441** | -0.437** | -0.405** | -0.425** | -0.448** | -0.418** | -0.413** |
| PCPHE | -0.000 | -0.078 | -0.190 | -0.140 | -0.309 | -0.218 | -0.427** | -0.498** | -0.452** | -0.457** | -0.454** |
| AHCR | -0.261 | -0.184 | -0.104 | -0.125 | -0.15 | -0.132 | -0.12 | -0.133 | -0.112 | -0.168 | -0.165 |
| UR | -0.489** | -0.437** | -0.493** | -0.537** | -0.535** | -0.541** | -0.522** | -0.512** | -0.524** | -0.550*** | -0.546*** |
| EQI | -0.500** | -0.416** | -0.235 | -0.404** | -0.477** | -0.370** | -0.372 | -0.178 | -0.327* | -0.251 | -0.260 |
Note: ***p<0.001;** p<0.05;* p<0.1 |
Table 2 Key human factor parameters estimated using SDM |
| Variable | Elastic coefficient | T value | P value | Variable | Elastic coefficient | T value | P value |
|---|---|---|---|---|---|---|---|
| lnGDPPC | -0.017** | -2.39 | 0.017 | W*lnGDPPC | -0.037*** | -2.79 | 0.005 |
| lnPCPHE | -0.013** | -1.98 | 0.049 | W*lnPCPHE | 0.003 | 0.48 | 0.630 |
| lnAHCR | -0.054 | -1.36 | 0.174 | W*lnAHCR | 0.029*** | 2.83 | 0.005 |
| lnUR | -0.129** | -2.32 | 0.021 | W*lnUR | 0.093*** | 3.40 | 0.001 |
| lnEQI | -0.012** | -2.08 | 0.035 | W*lnEQI | -0.081*** | 3.99 | 0.000 |
| W*lnRHI | 0.030*** | 3.51 | 0.001 |
Note: *** p<0.01; ** p<0.05;* p<0.1; W* lnGDPPC, W* lnPCPHE, W* lnAHCR, W* lnUR and W* lnEQI stand for the spatial lagging of GDPPC, PCPHE, AHCR, UR, and EQI respectively. |
Table 3 Estimates of key human factors direct and indirect effects |
| Variable | Direct effect | P value | Indirect effect | P value |
|---|---|---|---|---|
| lnGDPPC | -0.018** | 0.038 | -0.164*** | 0.009 |
| lnPCPHE | -0.016** | 0.045 | 0.009 | 0.747 |
| lnAHCR | -0.057 | 0.180 | 0.125** | 0.015 |
| lnUR | -0.132** | 0.021 | 0.410*** | 0.001 |
| lnEQI | -0.008** | 0.011 | -0.362*** | 0.000 |
Note: *** p<0.01; ** p<0.05; * p<0.1 |
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
Commission on Social Determinants of Health (WHO CSDH), 2008. Closing the gap in a generation: Health equity through action on the social determinants of health. .
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
National Health and Family Planning Commission (NHFPC), 2015. China Statistical Yearbook of Health and Family Planning (2015). Beijing: Chinese Union Medical University Press . (in Chinese)
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
UNU-EHS (United Nations University, Institute for Environment and Human Health), IHDP, 2008. Towards sustainable global health. Source-Publication Series of UNU-EHS, 11.
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}